Abstract
This research is a quantitative survey study which explored attitudes of American nurses regarding circumcision and the care of the non-circumcised client (intact care). The descriptive study was conducted to examine current nursing perspectives in light of nationally declining routine infant circumcision in the United States. Watsons Theory of Human Caring was utilized as a framework for this investigation. Data was collected via an anonymous survey distributed via social media, with a convenience sampling method yielding an n=345. Results were analyzed using frequencies and Pearsons correlations with no significant findings. With no discernable patterns in nurse responses to items regarding their attitudes on circumcision and care of the intact client, the focus of clinical practice is placed on personal introspection and provision of care that is congruent with cultural competence and caring principles.
Keywords: circumcision, intact care, Watson Theory of Human Caring, nurse attitudes
Introduction
Routine infant circumcision (RIC) has been declining in the United States (US) for the past thirty years, and rates are widely variable based on region of the country (Center for Disease Control and Prevention, 2011; Owings, Uddin & Williams, 2013). The CDC (2011) reported national circumcision rates at 58.3% most recently, down from 64.5% in the late 1970s. Congruent with this trend, genital integrity has gained attention among American parents, with some states having minimal practice of the procedure, particularly where federal health programs no longer offer reimbursement (Na, Tanny & Hudson, 2015). Contributing factors may include the ethnic and religious composition of differing regions, and beliefs regarding hygiene.
Presently, in regions of the US, newborn circumcision rates can still exceed 80% (CDC, 2011). Trends in rates of RIC have also been historically impacted by the issuance of position statements by American Academy of Pediatrics (AAP) (2012) which issued the most recent revision of its position statement on RIC in 2012, indicating that while the AAP found there to be benefits to the procedure, these benefits were insufficient to routinely recommend circumcision for all male infants.
Background
Relative to this cultural phenomenon, American nurses are likely to encounter a greater number of intact (non-circumcised) male clients in their practice, necessitating nursing care that is safe, accurate and respectful to the personal preferences of the client. The AAP statement acknowledges that parental choice should be of chief consideration in the circumcision decision (2012). Potential benefits put forth in this statement include the reduction of certain cancers, urinary tract infections in infancy and the reduction in sexually transmitted infections (AAP, 2012). This statement has been rebuked by world medical organizations as culturally biased (Frisch, 2013). Previous beliefs regarding infection incidence and prevention of cancers have been contested in recent literature (Svobda, 2017). Meta-analysis data suggests the need to perform more that 110 circumcisions to prevent a single urinary tract infection)Singh-Grewal, Macdessi & Craig, 2005). Discussion in the medical literature is contradictory.
There is minimal discussion of the concept of intact care in American medicine. Intact care refers to appropriate hygiene and procedural care of foreskin. Current nursing practices are not always reflective of evidence-based intact care. This is problematic, as inappropriate care of the foreskin, particularly in infants and children can lead to complications such as bleeding, scarring, infection, and pain (Krill, Palmer & Palmer, 2011).
The need for nursings sensitivity in caring for clients of varying opinions and decisions on this issue is magnified under the emerging view of clients as customers of the health industry, who have consumer power in their choices of when and where to access health services (Vogus & McClelland, 2016). American clients are becoming increasingly engaged and informed health consumers, who may carry strong opinions and rationales for their health choices (Washington, 2014). Patient perceptions of healthcare provider attitudes can be impactful in their health decision making. The delivery of poor-quality care and experience to these consumers has high costs for health systems and patient outcomes, particularly in diverse patient populations (Vogus & McClelland, 2016).
Among all health professions, nursing has the most direct patient interaction (DeLucia, Ott, & Palmieri, 2009). The scope of practice for nursing involves caring for the entire patient, including their lived experience of health or illness, nurses are frequently responsible for providing care of an intimate or personal nature, including hygiene, and performing somewhat invasive procedures such as urinary catheterization. In carrying out these practices, nursing professionals embrace efforts to offer respectful, personal and family-centric care. This family-centric model best serves clients and their families (Coyne, 2015). The formation of trusting nurse-client relationships can promote optimal outcomes. In the professional setting, clients more freely share information with providers whom they trust (Allinson & Chaar, 2016).
Significance
Despite nursings natural predisposition to this person-centered approach, the formation of a therapeutic relationship between the nurse and client can be hindered by a number of issues. In studies examining factors impacting the physician-client relationship, provider attitude has been implicated as a factor that can impact the patients transparency in communication (Flickinger et al. 2016) and the overall quality of care received (Street, Gordon & Haidet, 2007). Attitude has been defined as having three major defining components including (a) a mental stateconscious or unconscious; (b) a value, belief, or feeling; and (c) a predisposition to behavior or action (Altmann, 2008).
In American nursing, particularly, attitude has been recognized as a key component in the improvement of quality and client-centered care by the Quality and Safety Education for Nurses (QSEN) initiative, a nationally recognized quality improvement program. According to QSEN, nurses must possess the knowledge, skills, and attitudes necessary for safe client care. A deficit in any of these areas can result in suboptimal client outcomes (QSEN, 2018).
In caring for the intact male client, attitudes of healthcare providers may be related to personal cultural or religious practices, previous education or routine practices that have been established in places of work. The avoidance of harm caused by traditional practices, and the ability to access safe health care has been asserted to be a human right and a key tenet of providing care that is culturally competent (Douglas et al.
2014). As American nurses see an increase in intact male clients in their practice environment, assessment of current attitudes regarding non-circumcision is needed to facilitate appropriate, culturally competent and person-centered nursing care to this often stigmatized population.
Methods
Theoretical Framework
Watsons Theory of Human Caring was utilized as a theoretical base for this work, as attitudes held by nurses can be of deep influence to the nurse-client relationship. The nurse-client domain is central to Watson’s theory, particularly in regards to the concepts of transpersonal caring, which describes a connection occurring between the nurse and client that is beyond physical and objective examination, and addresses how the caregiver approaches a client with reverence for their personal health experience (Watson as cited in Cara, 2003). This relationship is a mutual engagement that exists between the nurse and client, a reciprocal and overlapping connection that establishes the common goal for the protection of the client’s humanity and “inner harmony” (Cara, 2003). Approaching a patients personal and intimate health choices with this cognizance and respect is foundational to an effective nurse-client relationship as defined by Watson (1999). Addressing the health care needs of the client requiring intact care, pediatric or adult, both a respect for the clients choices and self-reflection are necessary. This must be further fortified by evidence-based knowledge of intact care guidelines.
Watsons caring science exists most pre-eminently in the nurse-client domain, where the vision of this theory is most evidently observed. In the interaction between nurse and client, particularly in the vulnerable and deeply personal moments nurses are often required to share with their patient, there is a need for human caring. This caring exists in the domain of the nurse, as Watson embraces this concept of caring as a transpersonal process, and in the caring relationship developed by the nurse and client (Watson, 1999). The concept of caring occasions/caring moments are developed within the setting in which transpersonal caring exist, and is defined by Watson as the moments in time when the nurse and client come together in situations that potentiate opportunities for human caring to occur (Watson, 1999). In this work, a previously held attitude or belief can impact this relationship, and ultimately enhance or impair the process and perception of caring, and is of greatest significance.
Additional concepts of Watson’s work with relevance to the research questions include: the Caritas Processes (originally described as carrative (i.e. caring) factors (Watson, 2008) of
(a) (a) “being authentically present and enabling and sustaining the deep belief system of self and one being cared for (p. 3 para 2)”; and
(b) (b) “reverently and respectfully assisting with basic needs with an intentional caring consciousness, administering human care essentials
which potentiate alignment of mind-body-spirit, wholeness and unity of being in all aspects of care” (Wagner, 2010).
The nurse must have a holistic mindset to adequately meet the needs of the population served, and must likewise have a deep sense of self-understanding and self-reflection to intervene in ways that are not only respectful but supportive of decisions surrounding health practices. The decision regarding circumcision may reflect beliefs that a client may consider as central to their sense of self, culture or faith. Watson’s work embodies this profound tolerance and obliges the nurse to emanate love and kindness in all interactions regardless of the nurses personal beliefs and views on the subject (Watson, 2008).
Design
This study was quantitative in design, with data being collected via anonymous, a web-based survey shared via social media. A primary ALT tool developed by the investigator was utilized due to a lack of availability of a valid and reliable measurement instrument.
Research Question
The primary purpose of this research was to explore the existing perceptions and attitudes of American nurses regarding the practice of routine infant circumcision and the intact client. The research questions that were utilized to guide the development of the primary investigator tool items were What are the attitudes and perceptions of American nurses regarding routine infant circumcision? and What are the attitudes of American nurses regarding care of the intact male client.
Sample
The research was designated as exempt by the institutional review board. No personally identifying data was collected. A convenience sample of 345 practicing American nurses was obtained through sharing of the survey link in social media communities for nurses. Participation in this research was voluntary, and a consent form was embedded in the survey sequence. This form informed respondents of their right to discontinue the survey at any time.
Nurse respondents were recruited via a social media survey link. Social media communities designed for nurses were identified through the social media host search function. Once a community was located, the primary investigator sent a direct message to the administrator of the group to request permission to post the survey link. Once permission was achieved, the link was posted to the group wall, with the investigators bumping the link every three to five days until the recruitment goal was achieved. In total, the link was posted in more the ten separate nurse-related social media groups. Participants did not have to like the post or comment on the post to participate. An embedded link took participants directly to the Qualtrics survey site for secure data collection. Internet protocol address tracking was disabled to protect the anonymity of respondents.
Results
In this investigation, participant attitude regarding RIC was assessed using a primary-investigator developed questionnaire with eight (8) statements that participants were asked to express agree, disagree or unsure in regards to survey items. A convenience sample of three hundred forty-five (n=345) nursing professionals were recruited via social media to participate in the study. Participants completed the survey via their personal devices, in their own environments. The research team never had direct contact with any of the anonymous participants. There was no intervention in this descriptive research.
Statistical Analysis
As this research investigation was descriptive in nature, there was no hypothesis to test. Data was examined using Pearsons correlations for relationships among items.
Outcomes
Of the three hundred forty-five participants, 334 (96.8%) participants identified as female, and 11 (3.2%) identified as male. The majority of the sample (n=315, 91.3%) identified as being Caucasian. The mean years of practice indicated by participants was 1 to 3 with experience levels ranging from pre-licensure to having practiced for more than 40 years. The mean age of respondents was 26 to 30 years old, with ages being reported from 18 to 25 to 66 or older. The most commonly identified area of practice of participants was inpatient hospital emergency department. The most commonly identified level of education was a bachelors degree in nursing science. Levels of education ranged from diploma to doctorate degree in nursing.
Data was analyzed using both frequencies for primary analysis and Pearsons correlations to examine for relationships among item responses. Frequency analysis is presented in Table 1.
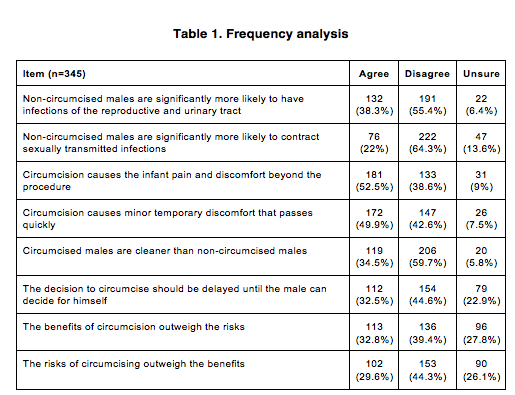
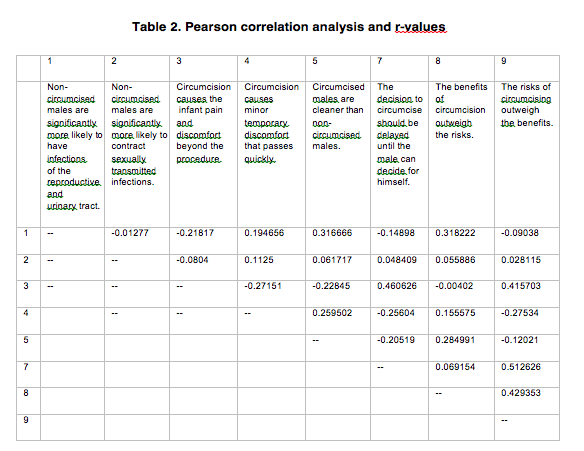
Upon analysis of frequency data, there was considerable variation in nurses responses to attitude items. No significant trends were noted with the evaluation of the data. Further analysis was conducted with Pearsons correlations for examination of potential relationships between item responses. Correlations are presented in Table 2.
Further analysis was conducted with Pearsons correlations for examination of potential relationships between item responses. Correlations are presented in Table 2.
In examining the correlation calculations, several significant relationships were recognized . Aa weak relationship (r = 0.3217) was noted between agreement with the survey item one, Non-circumcised males are significantly more likely to have infections of the reproductive and urinary tract, and an agreement with the survey item five, Circumcised males are cleaner than non-circumcised males. A weak relationship (0.3218) was additionally noted between agreement with survey item one and agreement with survey item nine, The benefits of circumcision outweigh the risks.
A weak to moderate correlation (0.461) between survey item three, Circumcision causes the infant pain and discomfort beyond the procedure and survey item seven, The decision to circumcise should be delayed until the male is old enough to decide for himself was also identified. Survey item three was found to additionally have a weak relationship (0.4216) to survey item nine The risks of circumcision outweigh the benefits. Survey items seven and nine were found to have a moderate correlation relationship of 0.513.
Lastly, the survey items nine and eight, The benefits of circumcision outweigh the risks had a correlation of
0.43 had a weak to moderate correlation of 0.430.
Discussion
This quantitative research sought to gain information about current attitudes of American nurses regarding non-circumcision and the intact client. This topic is timely, with rates of RIC declining on a national level (CDC, 2011). This survey was conducted via a shared social media link, with a n=345 individuals participating. An analysis was conducted by frequency and Pearsons correlations for relationships amongst survey items.
Frequency analysis demonstrated considerable variation in responses. No significant trend in responses could be discerned from the data available through this analysis. In examining correlations, relationships , though weak, were noted among items regarding cleanliness, infection risks and the belief that benefits of the procedure outweighed the associated risks. Conversely, relationships that were weak to moderate in strength were also noted between items regarding infant pain, the idea that the male should be allowed to choose if he desires to have the procedure done once he is at the age consent, and the belief that the risks of the procedure outweigh the benefits. The research team postulates that these divergent trends are likely associated with the deeply personal nature of beliefs regarding circumcision as a practice, the concepts of bodily autonomy and the issue of consent. Interestingly, the statement addressing the concept of consent, The decision to circumcise should be delayed until the male can decide for himself revealed nearly one in three nurses expressing agreement with this statement.
Additional research is needed to further explore these relationships, particularly factors that influence opinions regarding circumcision and care of the intact client. This could be achieved through further survey-type studies or focus groups. Further work would be benefitted by a greater diversity of respondents, as circumcision, and attitudes regarding this procedure, are likely to be influenced by culture, faith and geography.
Limitations
Limitations are acknowledged in this research. The methodology of recruiting participants through social media, though convenient, is limiting in that the population is inherently non-random. Additionally, using a computer-based recruitment strategy may inadvertently exclude potential participants who lack the ability or willingness to utilize social media. The most significant limitation was the lack of an established valid and reliable instrument to measure the phenomenon of interest. The use of a tool developed by the primary- investigator was therefore required. To account for this, the research team sought peer review of the survey prior to implementation. Despite this, the potential for bias cannot be excluded. Further limitations include the homogeneity of the sample group, which limits the generalizability of the research findings.
Recommendations for future research
The study findings and limitations give rise to a number of recommendations for future research. There is an opportunity to analyze the question regarding consent and the decision to delay male circumcision as areas of concern. This would prompt discussions regarding health care provider education about the evidence on pain experienced during the male circumcision procedure. Despite great advances in the understanding of infant pain and the lasting impact of early traumatic events, some healthcare providers continue to use no anesthetic in performing the circumcision procedure (Svodoba, 2017), as well as of any established benefits or harms. Nursing educators should focus on teaching the evidence-based and caring aspects of proper intact care, regardless of personal attitudes. In considering this, the education of the health care provider goes beyond the theoretical caring concepts. The knowledge will empower nurses to care holistically for intact clients in their roles and directly and indirectly affect patient safety.
Implications for Nursing Practice
With many nurses responding unsure to the survey items, there is an opportunity for professional introspection. In moving towards holistic care, a nursing approach which is caring and has a common goal of protecting the client’s concepts of body autonomy is an essential competency for all nurses. This concept requires caring for the clients body as they present it, rather than imposing the cultural norms or health care beliefs of the nurse upon it. Additionally, clinical knowledge of the anatomy and its appropriate care is an essential responsibility of nurses in all practice settings.
The phenomenon of caring is imperative as nurses strive to provide culturally competent client care.
Since the rates of RIC are declining in the US and as the needs of the American population change, client safety and culturally competent care are dependent on bedside nurses and other health care professionals having a nonbiased attitude regarding the clients intact or circumcised status and performing procedures and hygiene in ways that do not cause harm. Nurses should acknowledge the potential impact of personally held attitudes and beliefs regarding circumcision and non-circumcision on client care.
Recently legal challenges regarding female genital mutilation have been recognized as a violation of the human rights of girls and women (Baldas, 2018). This is prompting additional conversation regarding male circumcision and genital integrity. The national attention given to this issue has raised concerns regarding human rights to health, physical integrity and the right to be free from pain and discomfort (Earp, 2018).
Despite the controversy, nurses have an obligation to provide respectful and holistic care to clients of all beliefs. For these reasons, the primary caring change recommended is in the nursing attitude with which the principle of client care is transferred to the individual. When nurses show caring attitudes with rendering care to the intact client, they foster collaboration, enhancing the transpersonal caring relationship.
Conclusions
Nurses are the primary providers for face to face and direct client care at the bedside (DeLucia, Ott, & Palmieri, 2009) and frequently perform intimate care needs, like genital hygiene, incontinence care and urinary catheter care. With RIC rates declining in the US, American nurses will likely encounter intact clients more frequently, and will need to be culturally and clinically competent with providing client centered intact care. Provider attitude has been established as a factor impacting the provider-client relationship and client safety. Currently, nursing practice regarding intact care is inconsistent. In facilitating quality improvement, attitudes should be assessed and addressed, in addition to clinical knowledge and skills (QSEN, 2018).
Therefore, nursing attitude regarding circumcision and intact care were explored in this study with no significant trends identified.
Without having the ability to generalize attitudes among nurses, the focus should remain on personal introspection and nursings commitment to engaging in holistic client relationships such as described by Watson. The mutually inclusive nurse-client relationship is based upon the nurse’s moral commitment to connecting with clients, while the caring occasion/caring moment is the suitable time nurses find with clients for caring to occur. Regardless of an individual nurses opinions on circumcision, a commitment to providing care that is congruent with Watsons Theory of Human Caring will allow for transcendence of personal beliefs and optimization of client outcomes for the intact client.
Acknowledgements
This research did not require funding, and therefore does not require any funding disclosures. The authors do not have any conflicts of interest.
References
Allinson, M. & Chaar, B. (2016). How to build and maintain trust with patients. The Pharmaceutical Journal, 297: 7895. doi:20201862
Altmann, T. (2008). Attitude: A concept analysis. Nursing Forum, 43 (3), 144-150, doi: 10.1111/j.1744- 6198.2008.00106.x.
American Academy of Pediatrics Task Force on Circumcision. (2012). Circumcision policy statement. Pediatrics, 130 (3), 585.
Baldas, T. (November 20, 2018). Judge dismisses female genital mutilation charges in historic case. Detroit Free Press.
https:// www.freep.com/staff/27849/tresa-baldas/
Cara, C. (2001). A pragmatic view of Jean Watsons caring theory. Watson Caring Science Institute. http://watsoncaringscience.org/files/PDF/Pragmatic_View.pdf
Centers for Disease Control and Prevention, (2011). Trends in in-hospital newborn male circumcision — United States, 1999–2010. Morbidity and Mortality Weekly Report (MMWR) 60(34);1167-1168. CO: Westview Press, 1987.
Coyne, I. (2015). Families and health-care professionals’ perspectives and expectations of family-centered care: hidden expectations and unclear roles. Health Expect, 18: 796808. doi:10.1111/hex.12104
DeLucia, P. R., Ott, T. E., & Palmieri, P. A. (2009). Performance in Nursing. Reviews of Human Factors and Ergonomics, 5(1), 140. https://doi.org/10.1518/155723409X448008
Douglas, M.K. et al., (2014). Guidelines for implementing culturally competent nursing care. Journal of Transcultural Nursing, 25(2),109 121. doi:org/10.1177/1043659614520998
Flickinger, T. E., Saha, S., Roter, D., Korthuis, P. T., Sharp, V., Cohn, J., Moore, R. D., Ingersoll, K. S., Beach, M. C. (2015). Respecting patients is associated with more patient-centered communication behaviors in clinical encounters. Patient education and counseling , 99 (2), 250-5.
Frisch, M. et al. (2013). Cultural bias in the AAPs 2012 technical report and policy statement on male circumcision. Pediatrics, 131(4), p.796-800. doi:10.1542/peds.2012-2896
Krill A.J., Palmer, L.S., & Palmer, J.S. (2011). Complications of circumcision. Scientific World Journal. 11, 2458-2468. Na, A. F., Tanny, S. P. T., & Hutson, J. M. (2015). Circumcision: Is it worth it for 21st-century Australian boys? Journal of Pediatrics and Child Health, 51 (6), 58. doi.org/10.1111/jpc.12825
Owings, M., Uddin, S., & Williams, S., (2013). Trends in Circumcision for Male Newborns in U.S. Hospitals: 1979-2010. Retrieved from www.cdc.gov/nchs/data/hestat/circumcision_2013/circumcision_2013.pdf
Quality and Safety Education Safety for Nurses. (2018). About QSEN. Retrieved from http://www.qsen.org/about-qsen/ Singh-Grewal, D., Macdessi, J., Craig, J. (2005). Circumcision for the prevention of urinary tract infection in boys: A systematic review of randomized trials and observational studies. British Medical Journal, 90(8), 853-858.
Street, R.L, Gordon, H., Haidet, P. (2007). Physicians’ communications and perceptions of patients: is it how they look, how they talk, or is it just the doctor? Social Science Medicine. 65(3):586-98 doi:10.1016/j.socscimed.2007.03.036 Svoboda, J. S. (2017). Nontherapeutic circumcision of minors as an ethically problematic form of iatrogenic injury. AMA Journal of Ethics, 19(8), 815-824. doi: 10.1001/journalofethics.2017.19.8.msoc2-1708.
Vogus, T., & McClelland, L. (2016). When the customer is the patient: Lessons from healthcare research on patient satisfaction and service quality ratings. Human Resource Management Review, Volume 26, Issue 1, 2016, Pages 37-49 U.S. doi:10.1016/j.hrmr.2015.09.005
Wagner, A.L., (2010). Core concepts of Jean Watsons Theory of Human Caring/Caring Science. Watsons Caring Science Institute. http://www.watsoncaringscience.org/files/pdf/watsons-theory-human-caring-core-concepts-and- evoultion-to-caritas-processes-handout.pdf
Washington, L., (2014). Enabling consumer and patient engagement with health information. Journal of AHIMA, 85(2), 56-59.
Watson, J. (2008). Ten Caritas Processes. http://watsoncaringscience.org/about-us/caring-science-definitions- processes-theory/global-translations-10-caritas-processes/.
Watson, J. (1999). Postmodern nursing and beyond. Toronto, Canada: Churchill Livingstone
Attitudes of American Nurses Regarding Circumcision and Intact Care: A Survey Study
Attitudes of American Nurses Regarding Circumcision and Intact Care: A Survey Study
Volume 19, Number 1
Abstract
This research is a quantitative survey study which explored attitudes of American nurses regarding circumcision and the care of the non-circumcised client (intact care). The descriptive study was conducted to examine current nursing perspectives in light of nationally declining routine infant circumcision in the United States. Watsons Theory of Human Caring was utilized as a framework for this investigation. Data was collected via an anonymous survey distributed via social media, with a convenience sampling method yielding an n=345. Results were analyzed using frequencies and Pearsons correlations with no significant findings. With no discernable patterns in nurse responses to items regarding their attitudes on circumcision and care of the intact client, the focus of clinical practice is placed on personal introspection and provision of care that is congruent with cultural competence and caring principles.
Keywords: circumcision, intact care, Watson Theory of Human Caring, nurse attitudes
Introduction
Routine infant circumcision (RIC) has been declining in the United States (US) for the past thirty years, and rates are widely variable based on region of the country (Center for Disease Control and Prevention, 2011; Owings, Uddin & Williams, 2013). The CDC (2011) reported national circumcision rates at 58.3% most recently, down from 64.5% in the late 1970s. Congruent with this trend, genital integrity has gained attention among American parents, with some states having minimal practice of the procedure, particularly where federal health programs no longer offer reimbursement (Na, Tanny & Hudson, 2015). Contributing factors may include the ethnic and religious composition of differing regions, and beliefs regarding hygiene.
Presently, in regions of the US, newborn circumcision rates can still exceed 80% (CDC, 2011). Trends in rates of RIC have also been historically impacted by the issuance of position statements by American Academy of Pediatrics (AAP) (2012) which issued the most recent revision of its position statement on RIC in 2012, indicating that while the AAP found there to be benefits to the procedure, these benefits were insufficient to routinely recommend circumcision for all male infants.
Background
Relative to this cultural phenomenon, American nurses are likely to encounter a greater number of intact (non-circumcised) male clients in their practice, necessitating nursing care that is safe, accurate and respectful to the personal preferences of the client. The AAP statement acknowledges that parental choice should be of chief consideration in the circumcision decision (2012). Potential benefits put forth in this statement include the reduction of certain cancers, urinary tract infections in infancy and the reduction in sexually transmitted infections (AAP, 2012). This statement has been rebuked by world medical organizations as culturally biased (Frisch, 2013). Previous beliefs regarding infection incidence and prevention of cancers have been contested in recent literature (Svobda, 2017). Meta-analysis data suggests the need to perform more that 110 circumcisions to prevent a single urinary tract infection)Singh-Grewal, Macdessi & Craig, 2005). Discussion in the medical literature is contradictory.
There is minimal discussion of the concept of intact care in American medicine. Intact care refers to appropriate hygiene and procedural care of foreskin. Current nursing practices are not always reflective of evidence-based intact care. This is problematic, as inappropriate care of the foreskin, particularly in infants and children can lead to complications such as bleeding, scarring, infection, and pain (Krill, Palmer & Palmer, 2011).
The need for nursings sensitivity in caring for clients of varying opinions and decisions on this issue is magnified under the emerging view of clients as customers of the health industry, who have consumer power in their choices of when and where to access health services (Vogus & McClelland, 2016). American clients are becoming increasingly engaged and informed health consumers, who may carry strong opinions and rationales for their health choices (Washington, 2014). Patient perceptions of healthcare provider attitudes can be impactful in their health decision making. The delivery of poor-quality care and experience to these consumers has high costs for health systems and patient outcomes, particularly in diverse patient populations (Vogus & McClelland, 2016).
Among all health professions, nursing has the most direct patient interaction (DeLucia, Ott, & Palmieri, 2009). The scope of practice for nursing involves caring for the entire patient, including their lived experience of health or illness, nurses are frequently responsible for providing care of an intimate or personal nature, including hygiene, and performing somewhat invasive procedures such as urinary catheterization. In carrying out these practices, nursing professionals embrace efforts to offer respectful, personal and family-centric care. This family-centric model best serves clients and their families (Coyne, 2015). The formation of trusting nurse-client relationships can promote optimal outcomes. In the professional setting, clients more freely share information with providers whom they trust (Allinson & Chaar, 2016).
Significance
Despite nursings natural predisposition to this person-centered approach, the formation of a therapeutic relationship between the nurse and client can be hindered by a number of issues. In studies examining factors impacting the physician-client relationship, provider attitude has been implicated as a factor that can impact the patients transparency in communication (Flickinger et al. 2016) and the overall quality of care received (Street, Gordon & Haidet, 2007). Attitude has been defined as having three major defining components including (a) a mental stateconscious or unconscious; (b) a value, belief, or feeling; and (c) a predisposition to behavior or action (Altmann, 2008).
In American nursing, particularly, attitude has been recognized as a key component in the improvement of quality and client-centered care by the Quality and Safety Education for Nurses (QSEN) initiative, a nationally recognized quality improvement program. According to QSEN, nurses must possess the knowledge, skills, and attitudes necessary for safe client care. A deficit in any of these areas can result in suboptimal client outcomes (QSEN, 2018).
In caring for the intact male client, attitudes of healthcare providers may be related to personal cultural or religious practices, previous education or routine practices that have been established in places of work. The avoidance of harm caused by traditional practices, and the ability to access safe health care has been asserted to be a human right and a key tenet of providing care that is culturally competent (Douglas et al.
2014). As American nurses see an increase in intact male clients in their practice environment, assessment of current attitudes regarding non-circumcision is needed to facilitate appropriate, culturally competent and person-centered nursing care to this often stigmatized population.
Methods
Theoretical Framework
Watsons Theory of Human Caring was utilized as a theoretical base for this work, as attitudes held by nurses can be of deep influence to the nurse-client relationship. The nurse-client domain is central to Watson’s theory, particularly in regards to the concepts of transpersonal caring, which describes a connection occurring between the nurse and client that is beyond physical and objective examination, and addresses how the caregiver approaches a client with reverence for their personal health experience (Watson as cited in Cara, 2003). This relationship is a mutual engagement that exists between the nurse and client, a reciprocal and overlapping connection that establishes the common goal for the protection of the client’s humanity and “inner harmony” (Cara, 2003). Approaching a patients personal and intimate health choices with this cognizance and respect is foundational to an effective nurse-client relationship as defined by Watson (1999). Addressing the health care needs of the client requiring intact care, pediatric or adult, both a respect for the clients choices and self-reflection are necessary. This must be further fortified by evidence-based knowledge of intact care guidelines.
Watsons caring science exists most pre-eminently in the nurse-client domain, where the vision of this theory is most evidently observed. In the interaction between nurse and client, particularly in the vulnerable and deeply personal moments nurses are often required to share with their patient, there is a need for human caring. This caring exists in the domain of the nurse, as Watson embraces this concept of caring as a transpersonal process, and in the caring relationship developed by the nurse and client (Watson, 1999). The concept of caring occasions/caring moments are developed within the setting in which transpersonal caring exist, and is defined by Watson as the moments in time when the nurse and client come together in situations that potentiate opportunities for human caring to occur (Watson, 1999). In this work, a previously held attitude or belief can impact this relationship, and ultimately enhance or impair the process and perception of caring, and is of greatest significance.
Additional concepts of Watson’s work with relevance to the research questions include: the Caritas Processes (originally described as carrative (i.e. caring) factors (Watson, 2008) of
(a) (a) “being authentically present and enabling and sustaining the deep belief system of self and one being cared for (p. 3 para 2)”; and
(b) (b) “reverently and respectfully assisting with basic needs with an intentional caring consciousness, administering human care essentials
which potentiate alignment of mind-body-spirit, wholeness and unity of being in all aspects of care” (Wagner, 2010).
The nurse must have a holistic mindset to adequately meet the needs of the population served, and must likewise have a deep sense of self-understanding and self-reflection to intervene in ways that are not only respectful but supportive of decisions surrounding health practices. The decision regarding circumcision may reflect beliefs that a client may consider as central to their sense of self, culture or faith. Watson’s work embodies this profound tolerance and obliges the nurse to emanate love and kindness in all interactions regardless of the nurses personal beliefs and views on the subject (Watson, 2008).
Design
This study was quantitative in design, with data being collected via anonymous, a web-based survey shared via social media. A primary ALT tool developed by the investigator was utilized due to a lack of availability of a valid and reliable measurement instrument.
Research Question
The primary purpose of this research was to explore the existing perceptions and attitudes of American nurses regarding the practice of routine infant circumcision and the intact client. The research questions that were utilized to guide the development of the primary investigator tool items were What are the attitudes and perceptions of American nurses regarding routine infant circumcision? and What are the attitudes of American nurses regarding care of the intact male client.
Sample
The research was designated as exempt by the institutional review board. No personally identifying data was collected. A convenience sample of 345 practicing American nurses was obtained through sharing of the survey link in social media communities for nurses. Participation in this research was voluntary, and a consent form was embedded in the survey sequence. This form informed respondents of their right to discontinue the survey at any time.
Nurse respondents were recruited via a social media survey link. Social media communities designed for nurses were identified through the social media host search function. Once a community was located, the primary investigator sent a direct message to the administrator of the group to request permission to post the survey link. Once permission was achieved, the link was posted to the group wall, with the investigators bumping the link every three to five days until the recruitment goal was achieved. In total, the link was posted in more the ten separate nurse-related social media groups. Participants did not have to like the post or comment on the post to participate. An embedded link took participants directly to the Qualtrics survey site for secure data collection. Internet protocol address tracking was disabled to protect the anonymity of respondents.
Results
In this investigation, participant attitude regarding RIC was assessed using a primary-investigator developed questionnaire with eight (8) statements that participants were asked to express agree, disagree or unsure in regards to survey items. A convenience sample of three hundred forty-five (n=345) nursing professionals were recruited via social media to participate in the study. Participants completed the survey via their personal devices, in their own environments. The research team never had direct contact with any of the anonymous participants. There was no intervention in this descriptive research.
Statistical Analysis
As this research investigation was descriptive in nature, there was no hypothesis to test. Data was examined using Pearsons correlations for relationships among items.
Outcomes
Of the three hundred forty-five participants, 334 (96.8%) participants identified as female, and 11 (3.2%) identified as male. The majority of the sample (n=315, 91.3%) identified as being Caucasian. The mean years of practice indicated by participants was 1 to 3 with experience levels ranging from pre-licensure to having practiced for more than 40 years. The mean age of respondents was 26 to 30 years old, with ages being reported from 18 to 25 to 66 or older. The most commonly identified area of practice of participants was inpatient hospital emergency department. The most commonly identified level of education was a bachelors degree in nursing science. Levels of education ranged from diploma to doctorate degree in nursing.
Data was analyzed using both frequencies for primary analysis and Pearsons correlations to examine for relationships among item responses. Frequency analysis is presented in Table 1.
Upon analysis of frequency data, there was considerable variation in nurses responses to attitude items. No significant trends were noted with the evaluation of the data. Further analysis was conducted with Pearsons correlations for examination of potential relationships between item responses. Correlations are presented in Table 2.
Further analysis was conducted with Pearsons correlations for examination of potential relationships between item responses. Correlations are presented in Table 2.
In examining the correlation calculations, several significant relationships were recognized . Aa weak relationship (r = 0.3217) was noted between agreement with the survey item one, Non-circumcised males are significantly more likely to have infections of the reproductive and urinary tract, and an agreement with the survey item five, Circumcised males are cleaner than non-circumcised males. A weak relationship (0.3218) was additionally noted between agreement with survey item one and agreement with survey item nine, The benefits of circumcision outweigh the risks.
A weak to moderate correlation (0.461) between survey item three, Circumcision causes the infant pain and discomfort beyond the procedure and survey item seven, The decision to circumcise should be delayed until the male is old enough to decide for himself was also identified. Survey item three was found to additionally have a weak relationship (0.4216) to survey item nine The risks of circumcision outweigh the benefits. Survey items seven and nine were found to have a moderate correlation relationship of 0.513.
Lastly, the survey items nine and eight, The benefits of circumcision outweigh the risks had a correlation of
0.43 had a weak to moderate correlation of 0.430.
Discussion
This quantitative research sought to gain information about current attitudes of American nurses regarding non-circumcision and the intact client. This topic is timely, with rates of RIC declining on a national level (CDC, 2011). This survey was conducted via a shared social media link, with a n=345 individuals participating. An analysis was conducted by frequency and Pearsons correlations for relationships amongst survey items.
Frequency analysis demonstrated considerable variation in responses. No significant trend in responses could be discerned from the data available through this analysis. In examining correlations, relationships , though weak, were noted among items regarding cleanliness, infection risks and the belief that benefits of the procedure outweighed the associated risks. Conversely, relationships that were weak to moderate in strength were also noted between items regarding infant pain, the idea that the male should be allowed to choose if he desires to have the procedure done once he is at the age consent, and the belief that the risks of the procedure outweigh the benefits. The research team postulates that these divergent trends are likely associated with the deeply personal nature of beliefs regarding circumcision as a practice, the concepts of bodily autonomy and the issue of consent. Interestingly, the statement addressing the concept of consent, The decision to circumcise should be delayed until the male can decide for himself revealed nearly one in three nurses expressing agreement with this statement.
Additional research is needed to further explore these relationships, particularly factors that influence opinions regarding circumcision and care of the intact client. This could be achieved through further survey-type studies or focus groups. Further work would be benefitted by a greater diversity of respondents, as circumcision, and attitudes regarding this procedure, are likely to be influenced by culture, faith and geography.
Limitations
Limitations are acknowledged in this research. The methodology of recruiting participants through social media, though convenient, is limiting in that the population is inherently non-random. Additionally, using a computer-based recruitment strategy may inadvertently exclude potential participants who lack the ability or willingness to utilize social media. The most significant limitation was the lack of an established valid and reliable instrument to measure the phenomenon of interest. The use of a tool developed by the primary- investigator was therefore required. To account for this, the research team sought peer review of the survey prior to implementation. Despite this, the potential for bias cannot be excluded. Further limitations include the homogeneity of the sample group, which limits the generalizability of the research findings.
Recommendations for future research
The study findings and limitations give rise to a number of recommendations for future research. There is an opportunity to analyze the question regarding consent and the decision to delay male circumcision as areas of concern. This would prompt discussions regarding health care provider education about the evidence on pain experienced during the male circumcision procedure. Despite great advances in the understanding of infant pain and the lasting impact of early traumatic events, some healthcare providers continue to use no anesthetic in performing the circumcision procedure (Svodoba, 2017), as well as of any established benefits or harms. Nursing educators should focus on teaching the evidence-based and caring aspects of proper intact care, regardless of personal attitudes. In considering this, the education of the health care provider goes beyond the theoretical caring concepts. The knowledge will empower nurses to care holistically for intact clients in their roles and directly and indirectly affect patient safety.
Implications for Nursing Practice
With many nurses responding unsure to the survey items, there is an opportunity for professional introspection. In moving towards holistic care, a nursing approach which is caring and has a common goal of protecting the client’s concepts of body autonomy is an essential competency for all nurses. This concept requires caring for the clients body as they present it, rather than imposing the cultural norms or health care beliefs of the nurse upon it. Additionally, clinical knowledge of the anatomy and its appropriate care is an essential responsibility of nurses in all practice settings.
The phenomenon of caring is imperative as nurses strive to provide culturally competent client care.
Since the rates of RIC are declining in the US and as the needs of the American population change, client safety and culturally competent care are dependent on bedside nurses and other health care professionals having a nonbiased attitude regarding the clients intact or circumcised status and performing procedures and hygiene in ways that do not cause harm. Nurses should acknowledge the potential impact of personally held attitudes and beliefs regarding circumcision and non-circumcision on client care.
Recently legal challenges regarding female genital mutilation have been recognized as a violation of the human rights of girls and women (Baldas, 2018). This is prompting additional conversation regarding male circumcision and genital integrity. The national attention given to this issue has raised concerns regarding human rights to health, physical integrity and the right to be free from pain and discomfort (Earp, 2018).
Despite the controversy, nurses have an obligation to provide respectful and holistic care to clients of all beliefs. For these reasons, the primary caring change recommended is in the nursing attitude with which the principle of client care is transferred to the individual. When nurses show caring attitudes with rendering care to the intact client, they foster collaboration, enhancing the transpersonal caring relationship.
Conclusions
Nurses are the primary providers for face to face and direct client care at the bedside (DeLucia, Ott, & Palmieri, 2009) and frequently perform intimate care needs, like genital hygiene, incontinence care and urinary catheter care. With RIC rates declining in the US, American nurses will likely encounter intact clients more frequently, and will need to be culturally and clinically competent with providing client centered intact care. Provider attitude has been established as a factor impacting the provider-client relationship and client safety. Currently, nursing practice regarding intact care is inconsistent. In facilitating quality improvement, attitudes should be assessed and addressed, in addition to clinical knowledge and skills (QSEN, 2018).
Therefore, nursing attitude regarding circumcision and intact care were explored in this study with no significant trends identified.
Without having the ability to generalize attitudes among nurses, the focus should remain on personal introspection and nursings commitment to engaging in holistic client relationships such as described by Watson. The mutually inclusive nurse-client relationship is based upon the nurse’s moral commitment to connecting with clients, while the caring occasion/caring moment is the suitable time nurses find with clients for caring to occur. Regardless of an individual nurses opinions on circumcision, a commitment to providing care that is congruent with Watsons Theory of Human Caring will allow for transcendence of personal beliefs and optimization of client outcomes for the intact client.
Acknowledgements
This research did not require funding, and therefore does not require any funding disclosures. The authors do not have any conflicts of interest.
References
Allinson, M. & Chaar, B. (2016). How to build and maintain trust with patients. The Pharmaceutical Journal, 297: 7895. doi:20201862
Altmann, T. (2008). Attitude: A concept analysis. Nursing Forum, 43 (3), 144-150, doi: 10.1111/j.1744- 6198.2008.00106.x.
American Academy of Pediatrics Task Force on Circumcision. (2012). Circumcision policy statement. Pediatrics, 130 (3), 585.
Baldas, T. (November 20, 2018). Judge dismisses female genital mutilation charges in historic case. Detroit Free Press.
https:// www.freep.com/staff/27849/tresa-baldas/
Cara, C. (2001). A pragmatic view of Jean Watsons caring theory. Watson Caring Science Institute. http://watsoncaringscience.org/files/PDF/Pragmatic_View.pdf
Centers for Disease Control and Prevention, (2011). Trends in in-hospital newborn male circumcision — United States, 1999–2010. Morbidity and Mortality Weekly Report (MMWR) 60(34);1167-1168. CO: Westview Press, 1987.
Coyne, I. (2015). Families and health-care professionals’ perspectives and expectations of family-centered care: hidden expectations and unclear roles. Health Expect, 18: 796808. doi:10.1111/hex.12104
DeLucia, P. R., Ott, T. E., & Palmieri, P. A. (2009). Performance in Nursing. Reviews of Human Factors and Ergonomics, 5(1), 140. https://doi.org/10.1518/155723409X448008
Douglas, M.K. et al., (2014). Guidelines for implementing culturally competent nursing care. Journal of Transcultural Nursing, 25(2),109 121. doi:org/10.1177/1043659614520998
Flickinger, T. E., Saha, S., Roter, D., Korthuis, P. T., Sharp, V., Cohn, J., Moore, R. D., Ingersoll, K. S., Beach, M. C. (2015). Respecting patients is associated with more patient-centered communication behaviors in clinical encounters. Patient education and counseling , 99 (2), 250-5.
Frisch, M. et al. (2013). Cultural bias in the AAPs 2012 technical report and policy statement on male circumcision. Pediatrics, 131(4), p.796-800. doi:10.1542/peds.2012-2896
Krill A.J., Palmer, L.S., & Palmer, J.S. (2011). Complications of circumcision. Scientific World Journal. 11, 2458-2468. Na, A. F., Tanny, S. P. T., & Hutson, J. M. (2015). Circumcision: Is it worth it for 21st-century Australian boys? Journal of Pediatrics and Child Health, 51 (6), 58. doi.org/10.1111/jpc.12825
Owings, M., Uddin, S., & Williams, S., (2013). Trends in Circumcision for Male Newborns in U.S. Hospitals: 1979-2010. Retrieved from www.cdc.gov/nchs/data/hestat/circumcision_2013/circumcision_2013.pdf
Quality and Safety Education Safety for Nurses. (2018). About QSEN. Retrieved from http://www.qsen.org/about-qsen/ Singh-Grewal, D., Macdessi, J., Craig, J. (2005). Circumcision for the prevention of urinary tract infection in boys: A systematic review of randomized trials and observational studies. British Medical Journal, 90(8), 853-858.
Street, R.L, Gordon, H., Haidet, P. (2007). Physicians’ communications and perceptions of patients: is it how they look, how they talk, or is it just the doctor? Social Science Medicine. 65(3):586-98 doi:10.1016/j.socscimed.2007.03.036 Svoboda, J. S. (2017). Nontherapeutic circumcision of minors as an ethically problematic form of iatrogenic injury. AMA Journal of Ethics, 19(8), 815-824. doi: 10.1001/journalofethics.2017.19.8.msoc2-1708.
Vogus, T., & McClelland, L. (2016). When the customer is the patient: Lessons from healthcare research on patient satisfaction and service quality ratings. Human Resource Management Review, Volume 26, Issue 1, 2016, Pages 37-49 U.S. doi:10.1016/j.hrmr.2015.09.005
Wagner, A.L., (2010). Core concepts of Jean Watsons Theory of Human Caring/Caring Science. Watsons Caring Science Institute. http://www.watsoncaringscience.org/files/pdf/watsons-theory-human-caring-core-concepts-and- evoultion-to-caritas-processes-handout.pdf
Washington, L., (2014). Enabling consumer and patient engagement with health information. Journal of AHIMA, 85(2), 56-59.
Watson, J. (2008). Ten Caritas Processes. http://watsoncaringscience.org/about-us/caring-science-definitions- processes-theory/global-translations-10-caritas-processes/.
Watson, J. (1999). Postmodern nursing and beyond. Toronto, Canada: Churchill Livingstone
C/O National Alliance of Energy Healing
31907 South Davis Ranch Rd. Marana, AZ 85658
Email: ijhcjournal@earthlink.net Website: http://www.ijhc.org
Copyright © 2021 IJHC, NAOEP and Caitlin A. Connor. All rights reserved.
DISCLAIMER